
Medically reviewed by Jacques Lovely, RN, MN, MBA, PMP (Reg. #74334), Head of Western Operations, ATMA CENA.
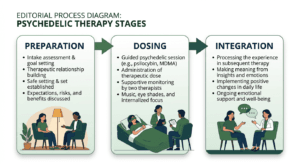
Integration is the structured therapy work that follows a psychedelic dosing session. In Canada, clinicians across ketamine, psilocybin, and MDMA-assisted therapy programs treat integration as a required clinical phase, not an optional follow-up. Published frameworks including PHRI (Gorman et al., 2021) and EMBARK (Brennan and Belser, 2022) describe what that work involves and why it determines whether a dosing experience translates into durable change.
Key takeaways
- Integration is the post-dosing phase of psychedelic-assisted therapy. Most clinicians treat it as the phase where durable change actually happens.
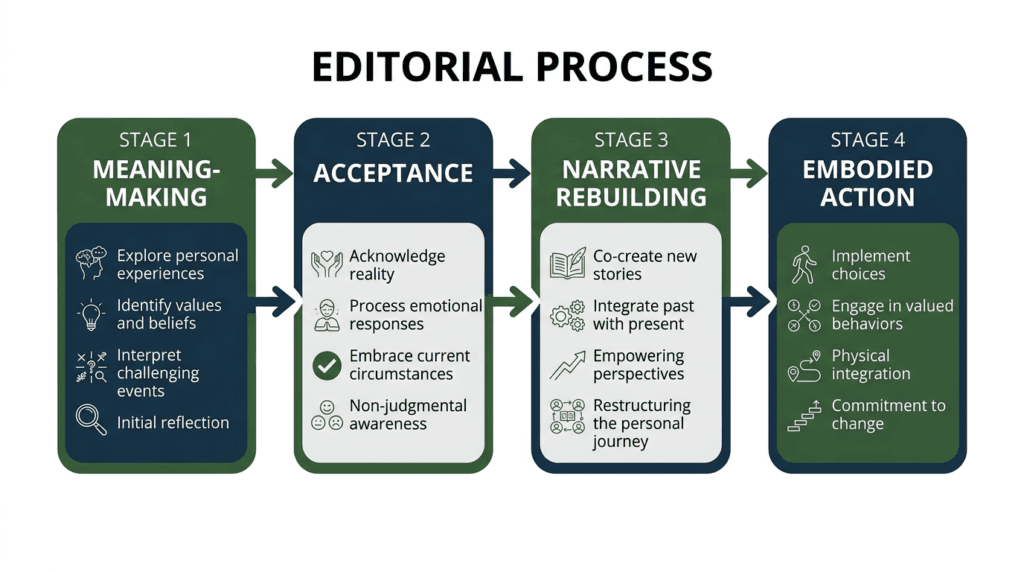
- The PHRI framework (Gorman et al., 2021) describes four integration domains: making meaning of the experience, accepting insights, building new narratives, and taking embodied action.
- The EMBARK framework (Brennan and Belser, 2022) adds six dimensions including ecological connection and relational integration, extending beyond symptom reduction to broader well-being.
- Typical timing: first integration session within 24–48 hours of dosing; then weekly sessions for 2–6 weeks. Substance, indication, and protocol determine exact session counts.
- The MDMA-AT protocols (Mitchell et al., 2021; Mitchell et al., 2023) included three integration sessions per dosing event. The COMP001 psilocybin protocol (Goodwin et al., 2022) included structured integration weeks after each dose.
- Ketamine integration is typically shorter and may be interleaved with ongoing dosing rather than concentrated after a single session.
- Skipping or under-attending integration is associated with earlier plateau and faster fading of initial response.
If you are weighing whether psychedelic-assisted therapy is right for your situation, book a free information call with ATMA CENA’s clinical team.

What Integration Is — and Why It Matters as Much as the Dose
Integration is the clinical and therapeutic process of moving material surfaced during a psychedelic dosing session toward durable change in how a person lives, thinks, and relates. It is not a debrief. It is not an interpretation of what the experience “meant.” It is structured psychotherapy, applied to material that arose during a pharmacological session.
The reasoning for treating integration as co-equal to dosing is straightforward. A psychedelic session can surface emotionally charged autobiographical material, previously unconscious patterns, somatic responses, and relational insights. Without structured therapeutic work, that material can fade, fragment, or remain unconnected to any change in behaviour or relationship. The dosing session opens the material; integration is what turns it into change.
This framing appears consistently in the integration literature. Earleywine et al. (2022) analysed definitions and methods from current integration providers and found meaning-making and behavioural translation to be the two most consistently named integration functions, with relationship quality between patient and therapist identified as central to integration quality.
The case is also structural. Mitchell et al. (2021), in the MAPP1 phase 3 MDMA-AT trial in 90 adults with severe PTSD, embedded three integration sessions following each of three dosing sessions. Goodwin et al. (2022), in the COMP001 phase 2b psilocybin trial in 233 adults with treatment-resistant depression, included integration weeks after each dosing session. Both trials showed clinically meaningful reductions in primary outcome measures. Neither framed the medication alone as the therapeutic mechanism.
The PHRI Framework: Four Domains of Integration Work
The Psychedelic Harm Reduction and Integration (PHRI) framework, published by Gorman et al. in 2021, was developed to describe the clinical tasks integration work addresses. It identifies four core domains.
Meaning-making is the work of putting the dosing experience into words and context, without imposing a “correct” interpretation. Reputable integration practice is non-prescriptive on meaning. The patient is the authority on what the experience meant; the clinician supports articulation and connection-making.
Acceptance involves supporting the patient to hold insights, emotions, or challenging material that arose during the session without suppressing or avoiding them. For some patients this is the most difficult integration domain, particularly where difficult or traumatic material surfaced.
Narrative rebuilding addresses the autobiographical stories patients carry about themselves, their relationships, and their circumstances. Material from dosing sessions often challenges established narratives. Integration helps patients build revised, more accurate, more adaptive accounts without the therapist directing what those accounts should be.
Embodied action is the translation domain, where integration most clearly distinguishes itself from a debrief. Insight in a dosing session is not, by itself, therapeutic. The therapeutic work is what changes: the conversation held, the boundary drawn, the pattern interrupted. Integration sessions identify candidate behaviour changes, troubleshoot obstacles, and follow up on whether they were attempted.
The EMBARK Framework: Six Dimensions of Integration
The EMBARK model, published by Brennan and Belser (2022), extends the integration frame beyond symptom reduction to include dimensions of well-being less commonly addressed in clinical trial endpoints. EMBARK is an acronym covering six dimensions: Embodied, Meaning-making, Belief systems, Aesthetic experience, Relational, and Key skills.
Where PHRI focuses on the clinical tasks integration accomplishes, EMBARK attends more explicitly to the experiential qualities of the psychedelic state and what they open therapeutically. Two dimensions are particularly worth naming for patients evaluating integration.
Relational integration addresses the interpersonal material that frequently surfaces during high-dose psychedelic sessions, including material about caregivers, partners, and formative relationships. Integration done without attending to this domain may leave relational insights unconnected to any change in how a person actually relates to others.
Meaning and belief systems addresses changes in existential orientation, values, or spiritual framework that some patients report following psychedelic sessions. These are not symptoms, but they are clinically significant. Patients who experience meaningful shifts in how they understand their lives benefit from structured space to examine and integrate those shifts, rather than returning to daily life without support for what has changed.
Both PHRI and EMBARK reflect the broader recognition in the integration literature that integration work requires psychotherapy training and competence, not merely the willingness to listen to a patient describe their experience.
When Integration Happens: Timing and Cadence
Timing of the first integration session is clinically significant. The practical consensus across published protocols and Canadian clinical practice is a first session within 24–48 hours of dosing, while the experience is freshest and material most accessible. Waiting longer than 72 hours risks loss of granular content and may leave patients without support during the period immediately following dosing.
After the first session, integration typically continues weekly for 2–6 weeks, with variation by substance and indication.
Key stat: In the MAPP1 trial (Mitchell et al., 2021), 90 adults with severe PTSD received three MDMA dosing sessions, each followed by three integration sessions. By the primary endpoint, 67% of the MDMA-group participants no longer met DSM-5 PTSD criteria, compared to 32% in the placebo group — in a protocol where integration was structurally embedded alongside the medication.
The integration cadence differs by substance:
MDMA-assisted therapy: The MAPP1 and MAPP2 protocols specified three integration sessions per dosing event. MDMA-AT involves long dosing sessions (6–8 hours) that typically surface substantial trauma-related autobiographical material; the integration load is accordingly high. MDMA remains accessible in Canada only through Health Canada’s Special Access Program on a case-by-case basis.
Psilocybin-assisted therapy: The COMP001 protocol included structured integration weeks following each dosing session. Psilocybin sessions are typically 5–6 hours and produce autobiographical, meaning-laden material that warrants sustained integration attention. Psilocybin remains a Schedule III controlled substance in Canada; access is through SAP only and is not guaranteed.
Ketamine-assisted therapy: Ketamine integration is typically shorter in total session count and may be interleaved with a multi-session dosing course. The acute dissociative experience tends to be less narratively rich than psilocybin or MDMA, so integration carries somewhat less autobiographical material to metabolize.
Note: ATMA CENA’s specific integration session counts per substance pathway should be confirmed at intake.
Approaches Used in Integration
No single modality is the correct one for integration work. Experienced Canadian clinicians typically draw from several frameworks depending on the patient and what arose during dosing.
Acceptance and Commitment Therapy (ACT) is a strong fit for the behavioural-translation function of integration. Watts and Luoma (2020) published a framework for using the psychological flexibility model to support PAT integration, arguing that ACT’s defusion and values-clarification components address the material psychedelic sessions commonly surface.
Internal Family Systems (IFS) is particularly used in MDMA-AT integration, attending to “parts” of the self — which maps well onto the material MDMA sessions frequently surface involving younger or wounded self-states.
Psychodynamic approaches are appropriate for material involving early-life patterns, attachment, and relational dynamics.
Somatic experiencing and body-based approaches attend to what the body holds, fitting for PTSD and somatic material from dosing sessions.
Group integration offers collective sense-making with witnessing and mutual support. In Canada, the Roots to Thrive program in Nanaimo, BC has published group-based PAT outcome data (Dames et al., 2025). Group integration is not suitable for every patient — the clinical decision between individual, group, or combined formats is made between patient and clinician.
Watch out: Patients who underestimate integration sometimes attend fewer sessions than recommended, believing the dosing session is “where it all happened.” The clinical pattern associated with under-attending integration is an earlier plateau in symptom improvement and faster fading of initial response gains. Integration is not the follow-up; it is part of the treatment.
How to Take the Next Step
If you are preparing for or have completed a psychedelic dosing session and want to understand what your integration phase should include, book a free information call with ATMA CENA’s clinical team.
For patients who already have a therapist they trust, integration does not have to happen outside that relationship. ATMA CENA’s CoCare model is designed so that long-term integration work happens with your existing therapist, with ATMA CENA providing the medication-specific coordination and dosing infrastructure.

Frequently Asked Questions
Why is integration described as the most important phase of psychedelic-assisted therapy?
Because durable change depends on it. The dosing session surfaces material; integration is the structured therapeutic process of moving that material into changed behaviour, revised narratives, and metabolized difficult experience. Published protocols including Mitchell et al. (2021) and Goodwin et al. (2022) embedded integration as a required phase, not an optional debrief.
What does PHRI stand for and what does it describe?
PHRI stands for Psychedelic Harm Reduction and Integration. Published by Gorman et al. in 2021, the framework describes four domains of integration work: making meaning of the experience, accepting insights, rebuilding narratives, and taking embodied action.
What is EMBARK and how is it different from PHRI?
EMBARK (Brennan and Belser, 2022) extends the integration frame to six dimensions: Embodied experience, Meaning-making, Belief systems, Aesthetic experience, Relational integration, and Key skills. Where PHRI focuses on clinical tasks, EMBARK attends more explicitly to experiential dimensions including relational and existential shifts. The two frameworks are complementary rather than competing.
How long is the integration phase?
Typically a first session within 24–48 hours of dosing, followed by weekly sessions for 2–6 weeks. Exact session counts depend on the substance, indication, and clinical model. The MDMA-AT phase 3 protocols included three integration sessions per dosing event. Psilocybin protocols included integration weeks after each session. Ketamine integration is typically shorter and interleaved with a multi-session dosing course.
Is integration optional?
No. Reputable Canadian psychedelic-assisted therapy programs treat integration as a required clinical phase. What the published protocols describe as psychedelic-assisted therapy includes integration as a structural component — omitting it does not constitute the same treatment.
What happens if I had a difficult or challenging experience during dosing?
A difficult experience is precisely what integration is for. Challenging material — including trauma, grief, or somatic discomfort that surfaced during dosing — is metabolized in integration over weeks, in a relationally safe therapeutic container with a trained clinician.
Can my existing therapist do my integration?
Yes, and this is what ATMA CENA’s CoCare model is designed for. Your existing therapist or psychiatrist remains the primary relationship; the psychedelic-specific integration layers on top with coordination from ATMA CENA’s clinical team.
Is group integration as effective as individual?
Group integration is a clinically reasonable format, particularly for sense-making and community-building functions of integration. Canadian evidence, including Dames et al. (2025) on the Roots to Thrive group model, supports group integration as an adjunct or, in selected populations, a primary format. Whether group, individual, or combined is the right approach is a clinical decision made between patient and clinician.
Does Spravato require integration?
The Health Canada label for Spravato (esketamine, approved for treatment-resistant depression in adults aged 18–64) does not require psychotherapy. Many Canadian Spravato programs nonetheless offer integration support, reflecting the clinical view that the therapeutic gains from medication are more durable when integration work accompanies dosing.
Compliance Disclaimer
Ketamine is approved by Health Canada as an anaesthetic. Use for depression, anxiety, PTSD, and other mental-health indications is off-label, regulated by provincial medical regulators — for example, CPSA in Alberta, CPSO in Ontario, and CPSM in Manitoba. Esketamine (Spravato) is Health Canada-approved for treatment-resistant depression in adults aged 18–64 as of May 2020.
Psilocybin and MDMA are restricted drugs under Canada’s Controlled Drugs and Substances Act. Patient access to psilocybin- or MDMA-assisted therapy is available only through Health Canada’s Special Access Program (SAP). SAP approval is granted on a case-by-case basis and is not guaranteed. Psilocybin SAP is primarily approved for adults with treatment-resistant major depressive disorder or distress associated with a life-threatening illness. MDMA SAP is primarily approved for adults with PTSD.
Nothing in this article should be construed as a clinical recommendation for a specific individual. Clinical decisions belong with a qualified prescribing physician.
About the Author
Reverdi Darda, RN, BScN (Reg. #61707) is CEO & Founder of ATMA CENA and a Registered Nurse with over three decades of experience in healthcare operations, community engagement, policy development, and strategic planning. A recognized leader in mental health access, Reverdi has dedicated her career to advancing evidence-based treatment models and advocating for policy change that prioritizes effective care. She founded ATMA CENA to expand practitioner and public access to psychedelic-assisted therapy across Canada.
Medically reviewed by Jacques Lovely, RN, MN, MBA, PMP (Reg. #74334), Head of Western Operations, ATMA CENA.
Sources
- Gorman, I. et al. (2021). Psychedelic Harm Reduction and Integration: A Transtheoretical Model for Clinical Practice. Frontiers in Psychology, 12, 645246.
- Brennan, W. & Belser, A.B. (2022). Models of Psychedelic-Assisted Psychotherapy: A Contemporary Assessment and an Introduction to EMBARK. Frontiers in Psychology, 13, 866018.
- Mitchell, J.M. et al. (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study (MAPP1). Nature Medicine, 27(6), 1025–1033.
- Mitchell, J.M. et al. (2023). MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial (MAPP2). Nature Medicine, 29(10), 2473–2480.
- Goodwin, G.M. et al. (2022). Single-Dose Psilocybin for a Treatment-Resistant Episode of Major Depression. New England Journal of Medicine, 387(18), 1637–1648.
- Earleywine, M. et al. (2022). Integration in psychedelic-assisted treatments: recurring themes in current providers’ definitions, challenges, and methods. Journal of Humanistic Psychology.
- Watts, R. & Luoma, J.B. (2020). The use of the psychological flexibility model to support psychedelic-assisted therapy. Journal of Contextual Behavioral Science, 15, 92–102.
- Dames, S. et al. (2025). Group-based psychedelic-assisted therapy in community mental health: outcomes from the Roots to Thrive program. Frontiers in Psychiatry.
- Health Canada (2022). Notice to stakeholders: Requests to the Special Access Program (SAP) involving psychedelic-assisted psychotherapy.