

Medically reviewed by Jacque Lovely, RN, MScN, MBA, Head of Western Operations, ATMA CENA.
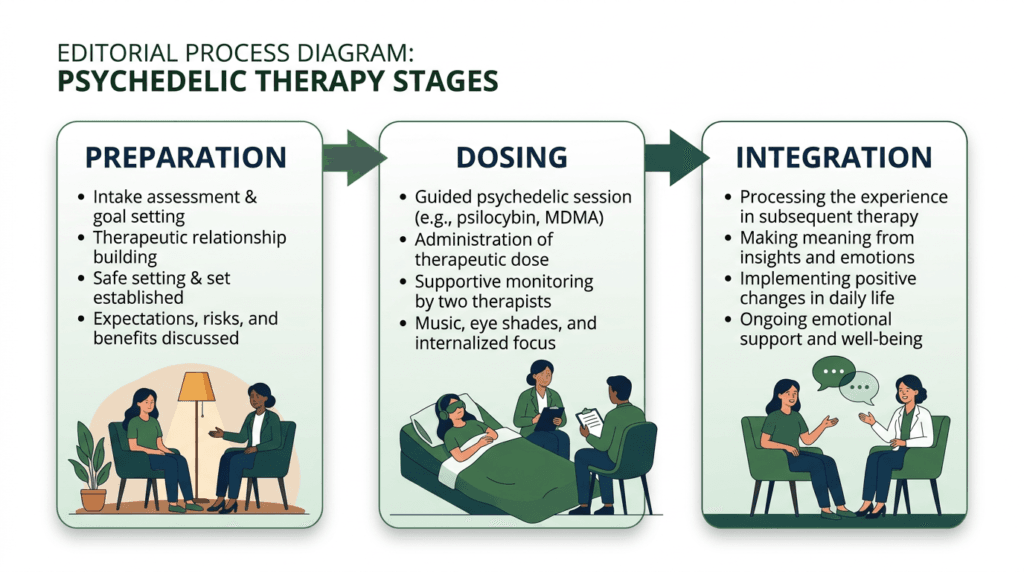
In Canada, psychedelic-assisted therapy is delivered in three phases: preparation, dosing, and integration. The preparation phase is the structured clinical work done before the first session — screening, alliance-building, medication review, intention-setting, and informed consent. It is not optional; it is the foundation on which safe and effective dosing depends.
Key takeaways
- Preparation accomplishes ten distinct clinical functions before any dosing occurs: intake, history review, medication review, therapeutic alliance, expectation-setting, psychoeducation, practical planning, grounding skills, intention-setting, and contraindication screening.
- Preparation length varies by substance: 1–3 sessions for ketamine; 2–4 sessions for psilocybin SAP; 3 structured sessions for MDMA-AT per the MAPP Phase 3 protocol.
- Medication review is clinically critical. SSRIs and SNRIs are generally tapered before psilocybin and MDMA dosing under medical supervision. MAOIs are an absolute contraindication for MDMA. Ketamine does not require antidepressant tapering.
- Patients must never stop, taper, or change psychiatric medications without the direct supervision of their prescribing physician.
- Poor preparation is associated with more difficult dosing experiences and weaker integration across the clinical literature.
- No amount of preparation guarantees a specific outcome. Response in psychedelic-assisted therapy remains individualized.
If you are evaluating whether psychedelic-assisted therapy is right for your situation, book a free 15-minute information call with ATMA CENA’s clinical team before you commit to anything.

What the Preparation Phase Is
The preparation phase is the first of three phases in the standard psychedelic-assisted therapy model: preparation, dosing, and integration. It encompasses every clinical encounter that happens before the patient enters a dosing session.
In Canada, this model is the standard frame across reputable programs delivering ketamine-assisted psychotherapy (KAP), psilocybin therapy under Health Canada’s Special Access Program (SAP), and MDMA-assisted therapy (MDMA-AT) under SAP. It originates in the MAPS MDMA-AT protocols (Mithoefer et al., 2011), the Imperial College London psilocybin trials (Carhart-Harris et al., 2016), and the COMPASS COMP360 psilocybin study (Goodwin et al., 2022).
Preparation is where the clinical team screens for contraindications, establishes trust with the patient, reviews and plans around medications, sets expectations, and builds the psychoeducation and psychological skills the patient will need in the dosing room. It is the part of the model most commonly under-resourced by lower-quality providers and most consistently correlated with better outcomes in the clinical literature.
What Preparation Accomplishes: Ten Clinical Functions
Preparation is not waiting-room time before the medicine. It is structured clinical work with ten distinct purposes.
1. Comprehensive Intake and Medical Screening
The preparation phase begins with a comprehensive intake: medical history (cardiovascular, endocrine, neurological, hepatic), surgical history, current medications and supplements, allergies, substance use history, and a structured psychiatric history. For ketamine and esketamine, blood pressure baseline and cardiovascular screening are routine. For psilocybin and MDMA, screening for personal and family history of psychotic disorders is non-negotiable.
2. Clinical History Review and Treatment Goals
The clinician reviews prior treatments — pharmacotherapy trials, psychotherapy modalities, dose adequacy, duration, response, and tolerability — and discusses what the patient is hoping to address. This anchors preparation in concrete, individualized goals rather than generic outcome talk.
3. Medication Review and Taper Planning
Medication review is one of the most clinically important components of preparation. How this plays out differs substantially by substance.
For psilocybin: SSRIs and SNRIs blunt the acute subjective intensity of psilocybin in a substantial proportion of users — approximately 50% of participants in self-report studies described attenuated effects. Multiple psilocybin clinical trials tapered antidepressants over 2–4 weeks with a minimum two-week washout before dosing (Goodwin et al., 2022; Carhart-Harris et al., 2021). A 2024 secondary analysis found a partial dissociation between acute psychedelic intensity and antidepressant outcome (Erritzoe et al., 2024) — a prospective RCT comparing taper versus continue has not yet been conducted as of 2026.
For MDMA: SSRIs and SNRIs attenuate MDMA’s subjective and therapeutic effects. The MAPP1 and MAPP2 Phase 3 protocols required supervised tapering and washout of psychiatric medications before the first experimental session (Mitchell et al., 2021; Mitchell et al., 2023). MAOIs are an absolute contraindication for MDMA due to the risk of life-threatening serotonin syndrome and hypertensive crisis — a minimum 14-day MAOI washout is required before any MDMA exposure.
For ketamine: SSRIs and SNRIs do not attenuate ketamine’s antidepressant effect and are generally continued during ketamine treatment (Veraart et al., 2021). Benzodiazepines above approximately 8 mg diazepam-equivalent daily have been shown to significantly reduce ketamine’s antidepressant effect and are sometimes held the day of dosing (Andrashko et al., 2020).
In all cases, the prescribing physician makes the taper decision. Patients must never stop, taper, or change psychiatric medications without the direct supervision of their prescribing physician.
4. Establishing Therapeutic Alliance
The patient meets the team present in the dosing session. In MAPP-style MDMA-AT protocols this is a co-therapy pair; in psilocybin protocols it is typically a lead therapist and co-therapist or sitter; in KAP it varies by clinic. The point of preparation is that the patient enters dosing having already established trust with the people in the room. Therapeutic alliance is one of the most consistent predictors of psychotherapy outcome across modalities (Flückiger et al., 2018).
5. Set and Setting
Preparation intentionally constructs both set (the patient’s mindset, expectations, intentions, and current state) and setting (the physical and relational environment of dosing). The set-and-setting framework, re-formalized by Hartogsohn (2017), is among the better-evidenced predictors of psychedelic experience quality. Leaving either to chance increases the likelihood of difficult experiences.
6. Trauma-Informed Psychoeducation
Patients are educated on what the substance does pharmacologically, what subjective effects to expect, and what kinds of phenomena — vivid imagery, emotion surfacing, body sensations, ego dissolution at higher psilocybin doses — are normal versus signals to communicate to the team. Trauma-informed framing reduces the likelihood that intense material in the dosing session is destabilizing rather than therapeutic.
7. Practical Planning
Preparation covers logistics: identifying a support person for transport and same-day care; confirming the patient cannot drive after dosing; booking a post-session day off work; scheduling the first integration appointment within 24–72 hours of dosing. Skipping practical planning is a common reason a clinically successful dosing session translates poorly into integration.
8. Anchor and Grounding Skills
Patients practise grounding skills — paced breathing, body scans, orienting techniques, simple somatic interventions — before dosing. These are the same skills available during the session if a difficult moment arises. Practising before the medicine is administered means the patient has the skill in their nervous system, not merely their head.
9. Intention-Setting
Intention-setting is the patient articulating what they hope to explore, change, or sit with during dosing. Intentions are specific to the patient’s goals and are not outcome promises. They become reference points during dosing and integration alike.
Pro tip: Intentions work best when they are specific and open rather than outcome-focused. “I want to look at the role of grief in my depression” is more useful than “I want to feel better.” The difference is one between inquiry and demand.
10. Safety and Contraindication Screening
Standard contraindication screens include: personal history of psychotic disorder; first-degree family history of psychotic disorder (especially for psilocybin and MDMA); uncontrolled cardiovascular disease; pregnancy and lactation; Bipolar I disorder (relative or absolute contraindication depending on substance and protocol); and active suicidal ideation with plan and means. A patient who does not meet safety criteria cannot be prepared into eligibility.
How Preparation Differs by Substance
Although the ten functions above apply across substances, preparation structure differs meaningfully by substance.
| Substance | Typical preparation sessions | Typical timeline | Psychotherapy emphasis |
|---|---|---|---|
| Ketamine (off-label KAP) | 1–3 sessions | 1–3 weeks | Moderate; increasing in evidence base |
| Spravato (esketamine) | Onboarding + 1–2 sessions | 1–2 weeks | Lower; label requires in-clinic monitoring |
| Psilocybin (SAP) | 2–4 sessions | 2–4 weeks | Substantial; COMP360-style protocol |
| MDMA-AT (SAP / MAPP-style) | 3 structured 90-minute sessions | 3–6 weeks | Heavy; MAPP1/MAPP2 protocol |
Ketamine and esketamine: KAP preparation has historically been 1–3 sessions, with less psychotherapy emphasis than psilocybin or MDMA protocols. The KAP literature increasingly documents outcome differences between psychotherapy-supported ketamine and infusion-only ketamine (Dore et al., 2019; Mathai et al., 2023).
Psilocybin SAP: Preparation in current Canadian SAP protocols is typically 2–4 sessions over 2–4 weeks with substantial psychotherapy emphasis, following COMP360-style structure (Goodwin et al., 2022).
MDMA-AT SAP: Preparation per the MAPP1 (Mitchell et al., 2021) and MAPP2 (Mitchell et al., 2023) protocols is 3 structured 90-minute preparation sessions with heavy emphasis on therapeutic alliance, trauma psychoeducation, and the inner-directed approach. MDMA-AT remains accessible in Canada only via Health Canada’s Special Access Program — SAP preparation generally follows MAPP-style protocols.
Note: ATMA CENA’s specific preparation session counts, duration, and sequencing per substance pathway should be confirmed at intake.

Why Preparation Matters: What the Evidence Shows
Three patterns recur across the controlled-trial and clinical-observation literature:
Poor preparation predicts difficult dosing experiences. Quality of set-and-setting, including the patient’s preparation and trust in the team, is among the better-evidenced predictors of subjective experience quality and acute-distress likelihood (Hartogsohn, 2017; Carbonaro et al., 2016). In a survey of 1,993 individuals describing their most psychologically difficult psilocybin experience, 84% nonetheless endorsed long-term benefit — but supervised, screened, and prepared participants have substantially better safety profiles than unsupervised users.
Poor preparation predicts weaker integration. Patients who enter dosing without articulated intentions, without practical post-session plans, and without alliance with the team report greater difficulty making sense of the experience and translating it into change.
Adverse events cluster in inadequately screened or prepared patients. Adverse-event reporting in psilocybin and MDMA RCTs concentrates in patients whose contraindication screening was suboptimal.
The COMP360 protocol (Goodwin et al., 2022), the MAPP1/MAPP2 protocols (Mitchell et al., 2021; Mitchell et al., 2023), and the original Mithoefer MDMA-AT protocols (Mithoefer et al., 2011) all build in 2–6 weeks of structured preparation for reasons supported by trial-level evidence rather than tradition.
What Preparation Does Not Do
- Preparation does not guarantee a good dosing experience. Even well-prepared patients can have challenging sessions. The team’s job is to support the patient through difficult material, not to prevent all difficulty.
- Preparation does not guarantee a good outcome. Response is individualized. The 25 mg psilocybin arm of the COMP360 trial showed 37% response and 29% remission at week 3 — meaningful, but not universal.
- Preparation cannot substitute for screening. A patient who does not meet safety criteria cannot be prepared into eligibility.
- Preparation cannot replace integration. Strong preparation makes integration possible; it does not perform integration in advance.
If you would like to talk through what the preparation phase would look like for your specific situation, book a free information call with ATMA CENA’s clinical team.

Frequently Asked Questions
How many preparation sessions will I have?
It depends on the substance, the clinic, and your clinical history. Typical ranges: 1–3 sessions for ketamine; 2–4 for psilocybin SAP; 3 structured sessions for MDMA-AT per the MAPP-style protocol. ATMA CENA calibrates preparation length to your specific substance, history, and goals — confirm at intake.
Can preparation sessions be done virtually?
Some components — intake interviews, history review, psychoeducation, intention-setting — can be conducted virtually. Other components, particularly grounding-skills practice with the dosing team and final clinical clearance, are typically in person. ATMA CENA’s CoCare model accommodates blended in-person and virtual preparation for patients with existing therapeutic relationships.
Do I need to taper my antidepressants before psychedelic-assisted therapy?
This is a clinical decision made by your prescribing physician — not a decision you should make on your own. For psilocybin and MDMA, most clinical trials required a supervised taper and washout of SSRIs and SNRIs before dosing. For ketamine and esketamine, most psychiatric medications continue concurrently. MAOIs are an absolute contraindication for MDMA. Patients must never stop, taper, or change psychiatric medications without the direct supervision of their prescribing physician.
What if I have a family history of psychotic disorders?
Family history of psychotic disorders is one of the most important screening criteria for psilocybin and MDMA. Personal history of psychosis is generally an absolute contraindication; first-degree family history is a strong relative contraindication, assessed case by case. Ketamine has a different evidence profile and is sometimes accessible in patients for whom psilocybin or MDMA is not.
Can my existing therapist be part of preparation?
Yes — this is what ATMA CENA’s CoCare model is built for. Your existing therapist or psychiatrist can remain the primary therapeutic relationship; preparation explicitly includes coordination with them where clinically appropriate. See ATMA CENA CoCare.
What is “set and setting” and why is it part of preparation?
“Set” is the patient’s mindset, expectations, intentions, and current state going into dosing. “Setting” is the physical and relational environment of the dosing session. The set-and-setting framework is among the better-evidenced predictors of psychedelic experience quality. Preparation is where both are intentionally constructed rather than left to chance.
What if I do not feel ready by the end of preparation?
Then the dosing session is rescheduled. Preparation that ends with the patient not feeling ready is preparation working as designed. Any provider who pressures a patient to dose before they feel ready is a clinical red flag.
Is preparation covered by insurance?
Coverage is substance- and program-specific. Spravato onboarding and preparation are often covered alongside the medication. KAP psychotherapy hours sometimes attract psychotherapy-benefit coverage. Psilocybin SAP and MDMA SAP are not generally covered by Canadian private insurance. See Insurance Coverage for Psychedelic-Assisted Therapy in Canada.
Why is preparation described as non-optional?
Every component of preparation has a specific clinical purpose: screening prevents harm; education reduces unhelpful surprise; intention-setting shapes the dosing experience; alliance-building supports difficult moments in the room; practical planning protects the post-session window; informed consent protects patient autonomy. A program that frames preparation as optional has not internalized the evidence base it claims to operate from.
Compliance Disclaimer
Psilocybin and MDMA are restricted drugs under Canada’s Controlled Drugs and Substances Act. Patient access to psilocybin- or MDMA-assisted therapy is available only through Health Canada’s Special Access Program (SAP). SAP approval is granted on a case-by-case basis and is not guaranteed. Psilocybin SAP is primarily approved for adults with treatment-resistant major depressive disorder or distress associated with a life-threatening illness. MDMA SAP is primarily approved for adults with PTSD.
Ketamine is approved by Health Canada as an anaesthetic. Use for depression, anxiety, PTSD, and other mental-health indications is off-label, regulated by provincial medical regulators — for example, CPSA in Alberta, CPSO in Ontario, and CPSM in Manitoba. Esketamine (Spravato) is Health Canada-approved for treatment-resistant depression in adults aged 18–64.
Nothing in this article should be construed as a clinical recommendation for a specific individual. Clinical decisions belong with a qualified prescribing physician.
About the Author
Reverdi Darda RN, BScN Reg # 61707 | CEO & Founder, ATMA CENA
Reverdi Darda, RN is CEO & Founder of ATMA CENA and a Registered Nurse with over three decades of experience in healthcare operations, community engagement, policy development, and strategic planning. A recognized leader in mental health access, Reverdi has dedicated her career to advancing evidence-based treatment models and advocating for policy change that prioritizes effective care. She founded ATMA CENA to expand practitioner and public access to psychedelic-assisted therapy across Canada.
Medically reviewed by Jacque Lovely, RN MN MBA PMP Reg# 74334 | Head of Western Operations at ATMA CENA
Sources
- Mitchell, J.M. et al. (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study (MAPP1). Nature Medicine, 27(6), 1025–1033.
- Mitchell, J.M. et al. (2023). MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial (MAPP2). Nature Medicine, 29(10), 2473–2480.
- Goodwin, G.M. et al. (2022). Single-Dose Psilocybin for a Treatment-Resistant Episode of Major Depression (COMP360). New England Journal of Medicine, 387(18), 1637–1648.
- Carhart-Harris, R.L. et al. (2016). Psilocybin with psychological support for treatment-resistant depression: an open-label feasibility study. Lancet Psychiatry, 3(7), 619–627.
- Carhart-Harris, R. et al. (2021). Trial of Psilocybin versus Escitalopram for Depression. New England Journal of Medicine, 384(15), 1402–1411.
- Mithoefer, M.C. et al. (2011). The safety and efficacy of MDMA-assisted psychotherapy in subjects with chronic, treatment-resistant PTSD. Journal of Psychopharmacology, 25(4), 439–452.
- Carbonaro, T.M. et al. (2016). Survey study of challenging experiences after ingesting psilocybin mushrooms. Journal of Psychopharmacology, 30(12), 1268–1278.
- Hartogsohn, I. (2017). Constructing drug effects: A history of set and setting. Drug Science, Policy and Law, 3, 1–17.
- Erritzoe, D. et al. (2024). Antidepressants blunt the subjective effects of psilocybin but do not fully predict antidepressant response. Journal of Psychopharmacology.
- Andrashko, V. et al. (2020). The antidepressant effect of ketamine is dampened by concomitant benzodiazepine medication. Frontiers in Psychiatry, 11, 844.
- Dore, J. et al. (2019). Ketamine Assisted Psychotherapy (KAP): Patient Demographics, Clinical Data and Outcomes in Three Large Practices. Journal of Psychoactive Drugs, 51(2), 189–198.
- Flückiger, C. et al. (2018). The alliance in adult psychotherapy: A meta-analytic synthesis. Psychotherapy, 55(4), 316–340.
- Veraart, J.K.E. et al. (2021). Ketamine treatment for depression: a review. Drugs, 81(14), 1659–1680.
- Health Canada (2022). Notice to stakeholders: Requests to the Special Access Program (SAP) involving psychedelic-assisted psychotherapy.
