
Canadian Registered Psychotherapists (CRPO Ontario), permit-holding psychothérapeutes (OPQ Quebec), and Master’s-level psychotherapists in other provinces are well-positioned to deliver the psychotherapy components of psychedelic-assisted therapy. This guide covers CRPO and OPQ scope, the legal landscape for the three substances (ketamine off-label, psilocybin SAP, MDMA SAP), continuing-education recognition, training programs in Canada, and how psychotherapists integrate into multidisciplinary PAT teams.
Key takeaways
- Registered Psychotherapists (RPs) hold the controlled act of psychotherapy in Ontario; OPQ permit-holders hold the equivalent restricted scope in Quebec. Both groups can legally deliver the psychotherapy components of PAT , preparation, in-session support, and integration , within authorized clinical-trial or SAP-approved programs [CRPO; OPQ Regulation C-26 r.222.1].
- RPs and psychothérapeutes cannot prescribe, administer, or possess any controlled substance, and cannot apply through Health Canada’s Special Access Program; SAP authority rests with physicians and nurse practitioners [CRPO; BCACC 2024].
- Ketamine-assisted therapy is the most accessible PAT context for psychotherapists today because ketamine is an approved medicine; psilocybin and MDMA require physician-led SAP applications.
- Health Canada’s December 2022 risk-management notice explicitly requires “a minimum of two therapists present” during dosing, with at least one “licensed to provide psychotherapy by a regulatory body.” RPs in Ontario and OPQ-permit psychothérapeutes in Quebec satisfy this requirement directly [Health Canada 2022].
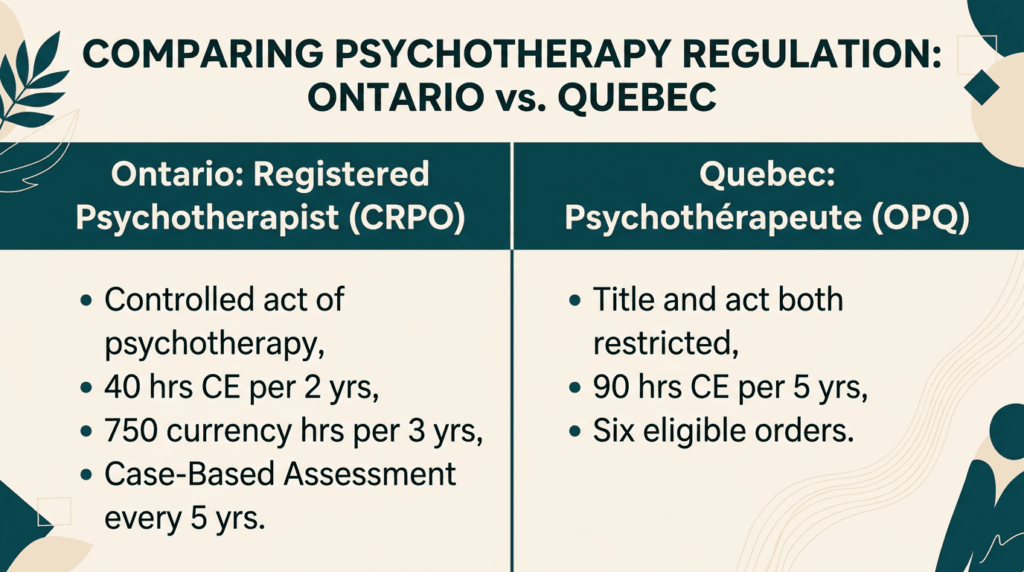
- CRPO’s Continuing Competency Program requires 40 hours of professional development per 2-year cycle (20 hours/year minimum) plus 750 currency hours per rolling 3-year period. OPQ permit-holders must complete 90 hours of CE in psychotherapy per 5-year period [CRPO; OPQ].
Not sure if the Clinical Pathway training fits your practice? Book a free information call & an advisor will walk you through eligibility, CE recognition, and next cohort dates.

Why Registered Psychotherapists are well-positioned for psychedelic work
Psychotherapists already hold the core competencies that PAT depends on: therapeutic alliance, trauma-informed framework, integration of altered or non-ordinary emotional states, and clinical attunement to set and setting. A meta-analysis of 295 studies (over 30,000 patients) confirms therapeutic alliance as a robust predictor of psychotherapy outcomes (r=0.278) [Flückiger et al. 2018]. In psilocybin trials specifically, stronger pre-session alliance predicted greater emotional breakthrough and lower depression scores at 4 weeks, 6 months, and 12 months post-treatment [Murphy et al. 2022; Levin et al. 2024]. Phelps’s foundational competency framework names empathetic abiding presence, trust enhancement, and self-awareness among the six core PAT competencies [Phelps 2017] , competencies psychotherapists develop throughout their training.
Specialized PAT training adds three layers on top of existing psychotherapy competence: substance-specific pharmacology and physiology, supervised medicine dosing-day skills, and the regulatory literacy to operate within Canadian frameworks (Health Canada SAP, provincial physician colleges, CRPO/OPQ scope rules). The Cavarra et al. (2022) systematic review of psychotherapy components across 26 PAT trials found that preparation, in-session support, and integration are universal structural features [Cavarra et al. 2022]; and psychotherapists are one of the professions that naturally deliver these components.
The legal landscape for psychotherapists in 2026
PAT in Canada operates under two distinct legal tracks for psychotherapists:
Ketamine-assisted therapy: ketamine is a Health Canada-approved anaesthetic prescribed off-label for psychiatric indications. Psychotherapists deliver the psychotherapy components within a multidisciplinary team led by a prescribing physician or nurse practitioner. Provincial physician colleges (CPSA Alberta, CPSM Manitoba, CPSBC BC, CPSO Ontario) set the operational rules [CPSA 2026; CPSM 2026; CPSBC 2025].
Psilocybin and MDMA: both remain restricted drugs accessible only through Health Canada’s Special Access Program. Psilocybin SAP is primarily granted for treatment-resistant major depressive disorder and end-of-life distress; MDMA SAP is primarily granted for PTSD [Health Canada 2022]. Psychotherapists cannot apply through SAP , the application must come from a prescribing physician or nurse practitioner. PsyCan documented an approximately 50 percent decline in SAP approvals through 2025, making this the more constrained pathway [PsyCan 2025].
CRPO neither endorses nor prohibits PAT for Ontario RPs but PAP-specific guidance [CRPO] is needed. Until that guidance is published, RPs operate under existing standards: the controlled act of psychotherapy applies (Standard 1.4), prescribing is outside scope, and competency expansion requires consultation and supervision (Standard 2.1).
CRPO requirements and competency expansion
CRPO’s Practice Standards (effective January 1, 2024) establish what RPs in Ontario can and cannot do in PAT contexts.
What RPs can do (per Standard 1.4.2): perform the controlled act of psychotherapy “provided they have the competence to do so in a safe and effective manner.” Authorized modalities include cognitive-behavioural, experiential and humanistic, somatic, psychodynamic, and systemic therapies , all relevant to PAT delivery.
What RPs cannot do (per Standard 1.4.1 and CRPO PAP resource): “RPs are not authorized to prescribe medication, give advice about medication or communicate a diagnosis.” RPs also cannot be in possession of illegal substances, cannot practise while impaired, must act within their area of competence, and must collaborate with care-team members.
Continuing Competency Program (Quality Assurance): – 40 hours of professional development per 2-year cycle (minimum 20 hours per year) – At least one didactic activity and at least one experiential activity per cycle – 750 currency hours of psychotherapy-related activities on a rolling 3-year basis – Self-assessment at least every two years – Case-Based Assessment approximately every five years (30 situational judgment cases, 80% pass)
CRPO does not maintain a list of accredited CE providers. PAT training programs (TheraPsil, Numinus, ATMA CENA) count toward the 40-hour requirement at the registrant’s judgment, provided the training is relevant to practice, credible, and documented.
CRPO’s PAP Resource Article explicitly directs registrants expanding into PAT to review Standard 2.1: Seeking Consultation, Clinical Supervision, and Referral. The Standard states that “knowing when to seek clinical supervision or consultation, and when to refer a client to another professional is integral to a registrant’s professional obligations.” Documenting consultation, supervision, and competency development is the professional record RPs maintain when expanding into PAT [CRPO Resource Article].
CRPO Standard 6.2 (Advertising) prohibits client testimonials, superlatives, comparisons to others, and outcome promises. RPs cannot advertise PAT services without verifiable training. Advertising must be “truthful, accurate, factual, and verifiable.”
The OPQ psychothérapeute pathway (Quebec)
In Quebec, both the title psychothérapeute and the act of psychotherapy are restricted under the Professional Code and the Regulation respecting the psychotherapist’s permit (C-26 r.222.1). The permit is issued by Ordre des psychologues du Québec (OPQ) to members of six regulated orders (guidance counsellors, occupational therapists, nurses, psychoeducators, social workers, marriage and family therapists). Physicians and psychologists practise psychotherapy under their own frameworks without a separate permit.
Authorized theoretical models under the regulation: psychodynamic, cognitive-behavioural, systemic, and humanist. PAT-relevant approaches (somatic, internal-family-systems, mindfulness-based, integration models) generally fit within these frameworks.
In a PAT context, Quebec psychothérapeutes can deliver preparation, in-session support, and integration psychotherapy as part of a physician-led team operating under SAP authorization or within an approved clinical trial. They cannot prescribe or administer.
Ready to see the full Clinical Pathway? Review course details, cohort dates, pricing, and CE credits for Registered Psychotherapists and allied mental-health clinicians.
Ketamine-assisted therapy: the most accessible clinical pathway
Ketamine is a Health Canada-approved anaesthetic prescribed off-label for depression, anxiety, PTSD, and chronic pain. Unlike psilocybin and MDMA, ketamine does not require SAP authorization. For psychotherapists, this makes ketamine-assisted therapy (KAT) the most immediately accessible PAT context after training.
Provincial-college rules govern the team and facility configuration. In Alberta, KAT delivered as part of psychedelic-assisted psychotherapy must occur in a CPSA-accredited facility with psychiatrist or physician-in-consultation oversight [CPSA 2026]. In British Columbia, non-IV ketamine routes are governed by CPSBC’s interim guidance v1.3 (August 2025) [CPSBC 2025]. In Manitoba, CPSM published current ketamine prescribing guidance in January 2026 [CPSM 2026]. In Ontario, CPSO has not issued a ketamine-specific policy.
Building a psychedelic practice within your existing registration
Trained psychotherapists integrate into PAT practice through three structures: clinical-trial sites, SAP-authorized programs led by a prescribing physician, or structured clinic-network models that handle medical and regulatory infrastructure.
ATMA CENA’s CoCare program is designed for the third structure. CoCare allows psychotherapists who have completed at least 50 hours of Clinical Pathway training to deliver preparation and integration psychotherapy in their own practice while ATMA CENA’s clinical infrastructure handles ketamine prescribing, dosing-day medical oversight, and facility compliance. Eligible designations include Registered Psychotherapists, Registered Clinical Social Workers, Registered Social Workers, and nurses in psychotherapy roles. Documentation, informed consent for off-label use, supervision arrangements, and liability coverage that explicitly includes PAT are professional-practice prerequisites psychotherapists arrange before active practice. CRPO Standard 1.5.1 and OPQ permit-holder rules require informed-consent documentation; off-label and SAP-context informed consent has additional disclosure requirements per CMPA’s March 2026 off-label drug guidance.
Training complete? Bring PAT into your existing practice. The CoCare model lets Registered Psychotherapists treat their own clients inside ATMA CENA clinics , maintaining the therapeutic relationship while accessing full medical infrastructure. Learn how CoCare works.

Frequently asked questions
Can a CRPO Registered Psychotherapist deliver psychedelic-assisted therapy in Ontario?
Yes , within the controlled act of psychotherapy and the CRPO scope rules. RPs can deliver preparation, in-session support, and integration psychotherapy as part of a multidisciplinary team led by a prescribing physician. RPs cannot prescribe, administer, or possess any controlled substance. CRPO is currently developing PAP-specific guidance; until published, registrants apply existing standards, particularly Standards 1.4 (Controlled Acts) and 2.1 (Consultation, Supervision, Referral) [CRPO].
Does a CRPO RP need specific accreditation to practise PAT?
CRPO does not require specific PAT certification for Ontario RPs as of May 2026. Practice within scope, with documented competency development through the 40-hr/2-yr Continuing Competency Program and ongoing supervision per Standard 2.1, satisfies CRPO’s professional-conduct requirements.
What’s the difference between a Registered Psychotherapist and a psychothérapeute under OPQ?
In Ontario, “Registered Psychotherapist” (RP) is the protected title under CRPO. In Quebec, “psychothérapeute” is the protected title under OPQ; the OPQ issues the psychotherapist’s permit to members of six regulated orders. Both are restricted titles in their respective provinces; Quebec additionally restricts the act of psychotherapy in a more granular way. The two regulatory frameworks differ but share similar scope outcomes: both groups can deliver psychotherapy within authorized PAT teams; neither can prescribe or administer.
What does the CRPO Continuing Competency Program require?
40 hours of professional development per 2-year cycle (minimum 20 hours per year), with at least one didactic and at least one experiential activity. RPs maintain 750 currency hours of psychotherapy-related activities on a rolling 3-year basis. Self-assessment occurs at least every two years; Case-Based Assessment occurs approximately every five years (30 situational-judgment cases, 80 percent pass). Annual attestation by March 31 [CRPO].
What happens after I complete training as a psychotherapist?
Trained psychotherapists join PAT delivery through clinical-trial sites, SAP-authorized programs led by a prescribing physician, or structured clinic-network models such as ATMA CENA’s CoCare. CoCare requires completion of at least 50 hours of Clinical Pathway training and provides clinical protocols, operational systems, and access to the network of trained clinicians.
Which ATMA CENA pathway is right for psychotherapists?
The Clinical Pathway is the primary route for RPs and OPQ permit-holders who will deliver the therapeutic components of PAT including dosing-day support. The Prescriber Pathway is for physicians and nurse practitioners and not applicable to psychotherapists.
Is personal psychedelic experience required to train?
Health Canada SAP protocols do not mandate personal psychedelic experience as a training prerequisite. The peer-reviewed argument for firsthand experience as a competency-relevant element [Dames et al. 2024] is one position in an active professional discussion rather than a settled clinical standard. Different programs make different choices on this question.
Sources
- CRPO. Practice Standards (effective January 1, 2024). https://crpo.ca/practice-standards/
- CRPO. Standard 6.2 Advertising. https://crpo.ca/practice-standards/business-practices/advertising/
- CRPO. Psychedelic-Assisted Psychotherapy Resource Article. https://crpo.ca/resource-articles/psychedelic-assisted-psychotherapy/
- CRPO. Quality Assurance Program Requirements. https://crpo.ca/registrant-information/registrant-requirements/quality-assurance-program/
- OPQ / Légis Québec. Regulation respecting the psychotherapist’s permit (C-26 r.222.1) (current January 1, 2026). https://www.legisquebec.gouv.qc.ca/en/document/cr/C-26,%20r.%20222.1%20/
- Health Canada (2022). Notice to stakeholders: SAP psychedelic-assisted psychotherapy. https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/announcements/requests-special-access-program-psychedelic-assisted-psychotherapy.html
- Health Canada (2022). Risk-management measures for clinical trials. https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/announcements/expectations-risk-management-measures-clinical-trials-psychedelic-assisted-psychotherapy.html
- CPSA (2026). Ketamine Prescribing, Administration and Oversight Expectations (March 2026). https://cpsa.ca/wp-content/uploads/2026/03/CPSA_Ketamine-Guidance_March-2026.pdf
- CPSA. Psychedelic-Assisted Psychotherapy Facility Accreditation. https://cpsa.ca/facilities-clinics/accreditation/psychedelic-assisted-psychotherapy/
- CPSM (2026). Ketamine: What Prescribers and Pharmacists Need to Know. https://www.cpsm.mb.ca/news/ketamine-what-prescribers-and-pharmacists-need-to-know
- CPSBC (2025). Interim Guidance v1.3 Ketamine non-IV routes. https://www.cpsbc.ca/files/pdf/IG-Ketamine-Administration-via-Intramuscular-Oral-Sublingual-Intranasal-Routes.pdf
- CAP Alberta (2025). Practice Guideline: Psychedelic-Assisted Psychotherapy (June 2025). https://www.cap.ab.ca/Portals/0/adam/Content/fQCpza4q7EGXC_psrgnCvA/Link/Psychedelic-Assisted%20Psychotherapy%20-%20June%202025.pdf
- BCACC (2024). Health Canada Guidelines on Psychedelic-Assisted Therapy. https://bcacc.ca/wp-content/uploads/2025/11/Health-Canada-Guidelines-on-Psychedelic-Assisted-Therapy-2024-October.pdf
- PsyCan (2025). Sharp Decline in Health Canada SAP Approvals (September 2025). https://psychedelicscanada.org/media/2025/09/psycan-discovers-sharp-decline-in-health-canada-approvals-for-doctors-seeking-legal-psychedelic-therapy-for-patients
- Flückiger, C. et al. (2018). The alliance in adult psychotherapy: meta-analytic synthesis. Psychotherapy, 55(4), 316–340. https://pubmed.ncbi.nlm.nih.gov/29792475/
- Murphy, R. et al. (2022). Therapeutic alliance and rapport modulate responses to psilocybin assisted therapy for depression. Frontiers in Pharmacology, 12, 788155. https://pmc.ncbi.nlm.nih.gov/articles/PMC9009076/
- Levin, A.W. et al. (2024). The therapeutic alliance and clinical outcomes in a psilocybin-assisted therapy trial. PLOS ONE, 19(3), e0300501. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0300501
- Phelps, J. (2017). Developing Guidelines and Competencies for the Training of Psychedelic Therapists. Journal of Humanistic Psychology, 57(5), 450–487. https://journals.sagepub.com/doi/10.1177/0022167817711304
- Tai, S.J. et al. (2021). Therapist Training Program for Psilocybin Therapy. Frontiers in Psychiatry, 12, 586682. https://pmc.ncbi.nlm.nih.gov/articles/PMC7908919/
- Cavarra, M. et al. (2022). Psychedelic-assisted psychotherapy: systematic review of associated psychological interventions. Frontiers in Psychology, 13, 887255. https://pmc.ncbi.nlm.nih.gov/articles/PMC9226617/
- Drozdz, S.J. et al. (2022). Ketamine Assisted Psychotherapy: Systematic Narrative Review. Journal of Pain Research, 15, 1691–1706. https://pmc.ncbi.nlm.nih.gov/articles/PMC9207256/
- Wilkinson, S.T. et al. (2017). Cognitive Behavior Therapy May Sustain Antidepressant Effects of IV Ketamine. Psychotherapy and Psychosomatics, 86(3), 162–167. https://pmc.ncbi.nlm.nih.gov/articles/PMC5516265/
- Yermus, R. et al. (2024). Ketamine-Assisted Psychotherapy at 3 and 6 Months. Psychedelic Medicine, 2(2), 87–95. https://pmc.ncbi.nlm.nih.gov/articles/PMC11613527/
- Mitchell, J.M. et al. (2021). MDMA-assisted therapy for severe PTSD: Phase 3 MAPP1. Nature Medicine, 27, 1025–1033. https://pmc.ncbi.nlm.nih.gov/articles/PMC8205851/
- Mitchell, J.M. et al. (2023). MDMA-assisted therapy for moderate to severe PTSD: Phase 3 MAPP2. Nature Medicine, 29, 2473–2480. https://www.nature.com/articles/s41591-023-02565-4
- Wang, J.B. et al. (2021). Multisite MDMA-AT scaling and fidelity. Journal of Humanistic Psychology. https://journals.sagepub.com/doi/full/10.1177/00221678211023663
- Goodwin, G.M. et al. (2022). Single-Dose Psilocybin for Treatment-Resistant Depression. NEJM, 387, 1637–1648. https://pubmed.ncbi.nlm.nih.gov/36322843/
- Raison, C.L. et al. (2023). Single-Dose Psilocybin for MDD. JAMA, 330(9), 843–853. https://pubmed.ncbi.nlm.nih.gov/37651119/
- Gorman, I. et al. (2021). Psychedelic Harm Reduction and Integration: Transtheoretical Model. Frontiers in Psychology, 12, 645246. https://pmc.ncbi.nlm.nih.gov/articles/PMC8008322/
- Brennan, W. & Belser, A.B. (2022). EMBARK: Transdiagnostic Trans-Drug Model. Frontiers in Psychology, 13, 866018. https://pmc.ncbi.nlm.nih.gov/articles/PMC9201428/
- Hartogsohn, I. (2018). Set and setting / meaning-enhancing properties. Frontiers in Neuroscience. https://pmc.ncbi.nlm.nih.gov/articles/PMC5845636/
- Modlin, N.L. et al. (2024). Trauma-Informed Care in Psychedelic Therapy Research. Neuropsychiatric Disease and Treatment, 20, 109–135. https://pmc.ncbi.nlm.nih.gov/articles/PMC10807282/
- Dames, S. et al. (2024). Firsthand experience as a training element. Psychedelic Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC11658659/